The Construction Quality Management (CQM) Methodology moves beyond the idea that quality managers are solely responsible for inspections and at fault for poor results. Informed by Human and Organizational Performance (HOP) best practices developed for the Department of Energy, CQM takes a holistic, integrated approach to construction quality, emphasizing systemic and organizational factors rather than individual blame.
Understanding Quality through a Holistic and Integrative Lens
CQM consistently presents a view where performance, including quality, is a systemic outcome rather than a collection of individual actions. This perspective is foundational to an effective CQM Methodology:
- Quality as a Systemic Property: Human Performance Improvement (HPI) and Integrated Safety Management (ISM) highlight that human performance is a system, comprising a network of elements that work together to produce repeatable outcomes, encompassing organizational factors, job-site conditions, individual behavior, and results. Applied to quality, this means construction quality is a direct reflection of the entire project system.
- Beyond Inspection: An Integrated Approach: CQM, like ISM, requires the involvement of management and workers at all organizational levels to integrate quality into work planning and execution. It is not merely a “program,” but a set of concepts and principles that aim to reduce errors and manage controls to eliminate unwanted events or mitigate their impact.
- Continuous Learning and Improvement: An effective CQM methodology must function as a learning organization, continuously monitoring performance, identifying deviations, self-assessing, and using quality analysis to improve. Learning from both successes and “information-rich, low consequence, no consequence events” (e.g., near misses, minor non-conformances) is crucial for preventing more significant quality failures.
“Bad” Quality Root Causes: Superficial and Blame-Oriented
CQM explicitly cautions against common pitfalls in identifying causes, which directly apply to superficial quality root causes:
- Human Error as a Symptom: A core principle is that human error is not the cause of failure, but rather the effect or symptom of deeper trouble in the system. Therefore, attributing poor quality solely to a quality manager’s inspection failures or the overall “Quality Management Program” being “bad” when test results are unsatisfactory, is a superficial and blame-oriented analysis [user query]. Such an approach often leads to blaming individuals for “bad decisions or inappropriate behavior” or for “failure to adhere to procedures”.
- Avoiding Symptomatic Attributions: Labels like “inattention to detail” or “not following procedures” are not root causes; they are behaviors that indicate underlying system weaknesses. When an investigation concludes that these are the causes, it fails to delve into why such behaviors occurred, thus preventing effective corrective actions.
- The “Bad Apple” Theory: This perspective assumes that problems are due to “inherent unreliability of people” and that removing “bad performers” will solve systemic issues. It overlooks that “people cannot perform better than the organization supporting them” and that “accidents result from a combination of factors, many of which are beyond the control of the worker”.
- The Blame Cycle: Blaming individuals for quality issues often leads to a “blame cycle” that reduces trust and communication, hindering the reporting of errors and near misses. This means deeper organizational weaknesses remain latent and unaddressed, perpetuating future problems.
“Common” Quality Root Causes: Systemic and Organizational
Effective quality root causes, aligned with the principles of HPI and ISM, are systemic and organizational deficiencies that, if corrected, would prevent the recurrence of the same or similar quality problems. These are “higher-order, fundamental causal factors that address classes of deficiencies, rather than single problems or faults”. They require a systematic analytical process to uncover the “why” behind the “what”.
These “common” quality root causes frequently represent failures in management systems to properly implement the core functions and guiding principles of safety and quality. They aim to identify latent organizational weaknesses—hidden deficiencies in management control processes or values that create error-provoking conditions or degrade controls.
Here are examples of Common Quality Root Causes, framed for a construction quality context:
- Deficiencies in Defining Work Scope and Requirements:
- Lack of clear or complete quality specifications: Failure to clearly define the expected quality outcomes, acceptance criteria, or performance objectives for construction tasks.
- Inadequate project planning: Errors in identifying critical quality-related steps, resources, or interfaces during the initial planning phase, leading to omissions in quality controls.
- Inadequate Hazard/Quality Risk Analysis:
- Failure to identify quality-critical activities or processes: Not recognizing specific construction activities or components where a deviation from expected quality could lead to significant consequences (e.g., structural integrity, critical system functionality).
- Overlooking “error precursors” for quality: Failing to anticipate conditions in the work environment (e.g., time pressure, high workload, confusing documentation, unfamiliarity with tasks) that increase the likelihood of quality defects.
- Ineffective Development and Implementation of Quality Controls:
- Flawed procedures or work instructions: Procedures that are technically incorrect, incomplete, or not user-friendly, making it difficult for workers to consistently achieve desired quality. This includes insufficient inclusion of human factors in procedure development.
- Inadequate staff competence or training: A lack of necessary technical knowledge, skills, or qualifications among personnel to perform quality-critical tasks.
- Insufficient resource allocation for quality: Budgetary or scheduling decisions that do not provide adequate time, qualified personnel, or appropriate tools/equipment for quality assurance and control activities.
- Ambiguous roles and responsibilities for quality assurance (QA) and quality control (QC): Lack of clear delineation of who is responsible for specific quality checks, approvals, or issue resolution.
- Failures in Work Execution within Quality Controls:
- Significant “Work-as-Planned” vs. “Work-as-Done” Gap (ΔWg): A systematic discrepancy between documented quality plans/procedures and actual practices in the field. This indicates that the planned controls are not being effectively implemented or are not realistic for the work environment.
- Lack of “Questioning Attitude” regarding quality: Individuals failing to challenge discrepancies, unclear instructions, or perceived shortcuts that could impact quality.
- Ineffective communication during work: Breakdown in sharing critical quality-related information or concerns among team members, supervisors, and other stakeholders.
- Ineffective Feedback and Continuous Improvement Systems for Quality:
- Failure to learn from “Operating Experience” (OE): Not systematically collecting, analyzing, and applying lessons learned from internal or external quality incidents, near misses, or best practices.
- Weak self-assessment and independent oversight mechanisms: Lack of rigorous internal or external reviews to identify latent quality weaknesses, verify control effectiveness, and track corrective actions to closure.
- Ineffective problem reporting and corrective action programs: Systems that do not encourage prompt and open reporting of quality issues and near misses, or where identified problems are not thoroughly analyzed and resolved with verified effectiveness.
- Unhealthy Organizational Culture Regarding Quality:
- Misalignment of values and priorities: When production or schedule goals implicitly or explicitly override quality considerations, sending “mixed signals” to the workforce.
- Lack of a “Just Culture” for quality: Punishing individuals for honest quality errors, which discourages reporting and prevents the organization from learning from its mistakes.
- Complacency or arrogance: A belief that past successes guarantee future quality outcomes, leading to resistance to new methods or a lack of vigilance.
- Insufficient management engagement: Line managers not actively involved in monitoring quality, coaching, mentoring, or demonstrating a commitment to high-quality performance in the field.
By utilizing this framework, a CQM methodology can effectively move beyond superficial blame and instead identify the systemic, organizational, and cultural factors that are the true root causes of quality issues, leading to more sustainable and impactful improvements in construction projects.
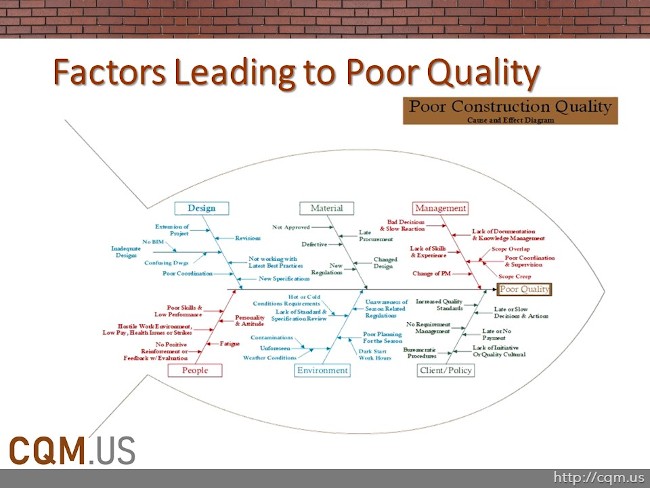
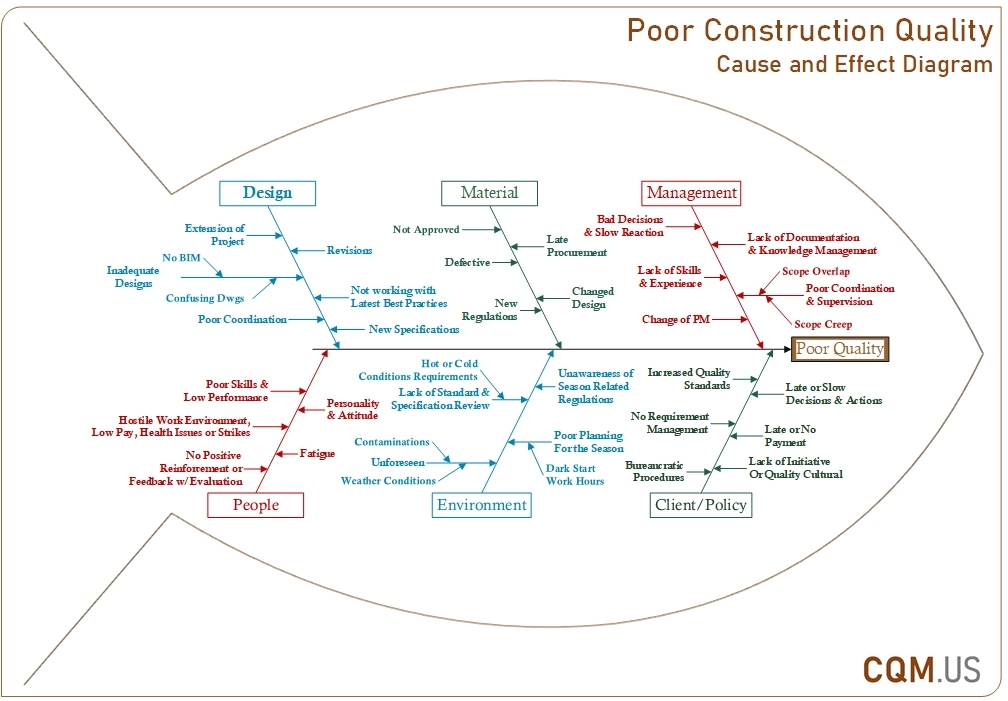
CQM Root Cause Fishbone
As many professional quality experts and project management professionals are familiar with the TQM Tools, Fishbone diagram or Ishikawa diagrams, developed by Kaoru Ishikawa, is the best visual display for causal diagrams. Dr. Hani Emari, PMP has developed a fishbone diagram to detect causes for poor quality in Construction and found that Poor Construction Project Outputs are due to the following factors:
- Poor Design & Engineering
- Poor Specification and/or Late Changes
- Inadequate Design and Poor Design Drawings
- Lack of Best Practices for Preventive measures (BIM)
- Too many Revisions and Poor Coordination
- Confusing Drawings and Irrelevant Information/Details
- Poor Supply of Material
- Submittal not approved properly
- Late Procurement with no advance preparation
- Late requirement Change and Substitution
- Unavailability of specified material or new Regulations
- Defective Material Delivered and not inspected
- Poor Project Management
- Not a Project Management Professional (CQM)
- Change in Project Management Team Personnel
- Bad Decisions made with slow responsiveness
- Poor Coordination and Lack of Supervision & Inspections
- Lack of Documentation and Knowledge Management
- Poor Manpower & People Performance
- Poor Skills, Lack of Training and Low Performance
- Hostile Work Environment, Health Issues, Low Pay, and Strikes
- Communication Barriers due to Personality Types, Cultures, Language and Attitude
- Fatigue and Exhaustion due to overwork
- No positive reinforcement, Feedback, or Evaluation
- Poor Environmental Controls
- Lack of consideration for Hot and Cold weather provisions
- Lack of Checklists for Specification and Standard Reviews
- Unaware of Seasonal Related Regulations and Conditions
- Poor Planning of Seasonal work, dark hours, and wrong season
- Contaminations and Unforeseen Environmental Conditions
- Poor Client Control and Lack of Policy
- Lack of Initiative for an IPD and Quality Culture Mindset
- Lack of Proper Scope and Requirement Management
- Late or No Payment to support the Cash Flow
- Lack of research and development prior to Architect selection
- Irrelevant and Overwhelming Industry Standard Requirements
Poor Specification is the Root Cause of Poor Quality
All the above factors contribute to the Poor Quality of Construction Production, however, the single most important cause that could help prevent almost all of the other factors is the project Specifications.
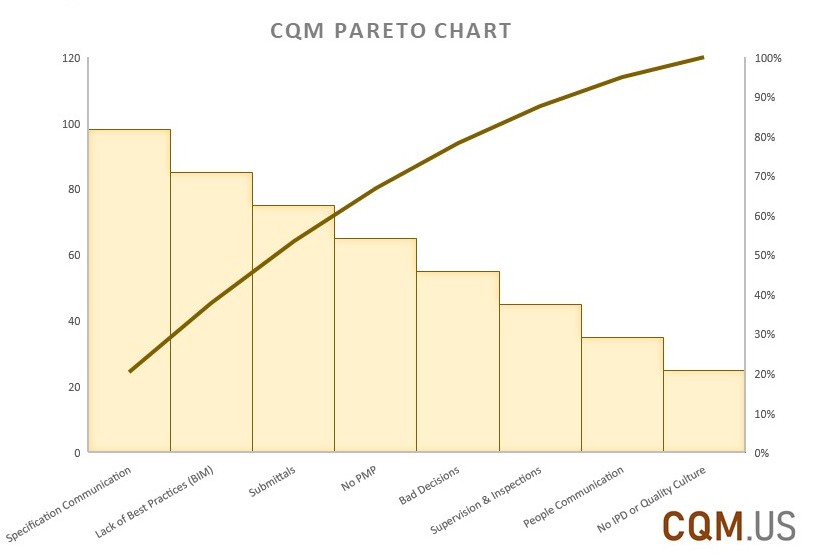
Project Specifications are the basis for Scope Management and Owner & A/E expectation of the final product. It drives the cost estimate and is the basis for the USACE CQM-C statement “Getting our money’s worth!” and contractors’ rebuttal of “You get what you paid for!” So the more irrelevant details and standard references are made by the A/E, the higher the cost of construction, and the less detail and industry standards are referenced, the fewer quality measures are monitored by the contractor. Therefore, highering the right Architect as the first step is the key to a high-quality construction product. Here are CQM Methodology’s recommendations for the Architects and Engineers:
- Be specific on why a section is provided and avoid irrelevant information and details
- Reference Standards with the reason why they are used, don’t include all possible standards and probable risk factors to transfer all risks which drive Cost unnecessarily high
- Provide Checklists of the most important Quality aspects concerned, whether it is a certain Material defect you are trying to avoid, equipment feature you desire, or environmental factor you are concerned with
- Provide portions of the Standard rather than the entire Standard Number
- Be collaborative and open with the Contractor rather than trying to be sneaky
- The specification is the Manual for what, why, how, when, where a material or activity must be performed, be clear and concise
- Use Specifications as a Communication Tool, don’t rely on others to decrypt your encrypted messages correctly if there is too much noise
The EIP (Energy Facility Contractors Operating Group) Accident Investigation, particularly as represented by the EIP-400 course and the underlying DOE handbooks, outlines a structured, comprehensive approach to understanding and preventing accidents. It moves beyond superficial causes to identify systemic and organizational deficiencies, aligning with a holistic and integrative approach to quality and safety.
What is the EIP Accident Investigation?
The EIP-400 course is an intermediate-level, performance-based simulation that illustrates the U.S. Department of Energy (DOE)’s investigative process for accidents. Its mission and purpose are to present an intensive accident investigation simulation covering roles, responsibilities, planning, teamwork, evidence collection and control, core analytical techniques, report writing, and quality reviews. This training meets the DOE O 225.1B Accident Investigation requirement for Federal Accident Investigation Board (FAIB) Chairpersons and DOE Accident Investigators, with full qualification obtained after participating in at least one FAIB. The course is also designed for DOE employees or contractors who wish to use these techniques for assessing and evaluating operations to prevent accidents and for continuous improvement.
The fundamental purpose of an accident investigation is to understand and identify the causes (both individual and organizational) that contributed to the accident so that deficiencies can be addressed and corrected to prevent recurrence and promote improved environmental protection, safety, and health. It also aims to promote the values and concepts of a learning organization, which continually monitors performance, identifies deviations, self-assesses, and uses quality analysis to improve. Investigations are expected to go “beyond the surface levels” to understand the “underlying sources of operational vulnerability”.
Methodology and Techniques
The EIP accident investigation process is complex and project-like, requiring careful planning, scheduling, and teamwork. It involves collecting, preserving, and verifying evidence; organizing and analyzing information; forming conclusions and Judgments of Need (JONs); and writing a final report. The overall process is iterative, meaning analyses are repeated and refined as new information becomes available.
The investigation framework and analytical process are designed to answer three primary questions:
- What happened?
- Why it happened?
- What to do to prevent re-occurrence?
To accomplish this, the methodology emphasizes several core analytical techniques:
- Events and Causal Factors (E&CF) Charting and Analysis
- Barrier Analysis
- Change Analysis
- Root Cause Analysis
- Verification Analysis
These techniques are mandatory for Federally-led investigations and highly recommended for contractor-led investigations and Operational Safety Reviews (OSRs).
1. Events and Causal Factors (E&CF) Charting and Analysis
The E&CF chart is considered the “backbone of the investigation”. It provides a graphical, chronological representation of events and conditions leading to an accident.
- Purpose: To consolidate and organize data, illustrate and validate the sequence of events, show relationships, identify information gaps, convey multiple causes, and guide report writing. It pinpoints specific events and conditions that, if addressed, would prevent recurrence.
- Process: Begins immediately and is continuously updated as information is collected. It reconstructs the primary chain of events chronologically, then adds secondary events and relevant conditions (environmental state or circumstance). Assumed events or conditions are noted with dotted lines. The analysis identifies significant events and conditions that led to the accident, moving from “what happened” to preparing for “why it happened”.
2. Barrier Analysis
Barrier analysis is a technique used to understand how hazards and targets interact and what controls failed.
- Purpose: To identify hazards associated with an accident and the barriers that should or could have prevented it, thus helping to identify potential causal factors and Judgments of Need (JONs). It operates on the premise that accidents occur when a hazard contacts a target due to barrier failure or non-use.
- Process: Involves identifying the hazard and target, then all relevant barriers (e.g., physical, management, administrative procedures, warning devices, knowledge/skills). Each barrier’s performance is evaluated, along with reasons for failure and how the failure affected the accident. It helps distinguish between barriers in place but failed, barriers not used, barriers not in place but required, and those that, if present, would prevent recurrence. The results are often documented in a Barrier Analysis Worksheet and integrated into the E&CF chart.
3. Change Analysis
Change analysis focuses on deviations from expected or planned situations that contributed to the accident.
- Purpose: To examine planned or unplanned changes that caused undesired outcomes, as change is a common factor in accidents that can be easily overlooked. It identifies obscure causal factors.
- Process: Involves describing the accident sequence, choosing and describing an “accident-free” or “ideal” situation (e.g., previous successful operation, design specifications, or documented procedures), comparing the two situations, identifying differences, analyzing their effect on the accident, and integrating the results into the E&CF chart. A Change Analysis Worksheet is used to structure this comparison. This includes comparing “work-as-planned” (management’s intent) versus “work-as-done” (actual practice) to identify significant gaps (ΔWg) that contributed to the event.
4. Root Cause Analysis
Root cause analysis is typically the final analytical task of an accident investigation and is crucial for preventing recurrence.
- Definition: Root causes are the causal factor(s) that, if corrected, would prevent recurrence of the same or similar accident(s). They are “higher-order, fundamental causal factors that address classes of deficiencies, rather than single problems or faults”.
- Types of Causes:
- Direct Cause: The immediate event(s) or condition(s) that caused the accident. There is only one direct cause for each accident.
- Contributing Causes: Events or conditions that, collectively with other causes, increased the likelihood of an accident but individually did not cause it.
- Local Root Cause: A specific deficiency whose correction would prevent the recurrence of the same accident.
- Systemic Root Cause: A management system deficiency whose correction would prevent the occurrence of a class of accidents. The investigation should aim to identify systemic root causes to address broader organizational issues.
- Process: Root cause analysis is not an exact science and requires judgment, ideally performed by the entire investigation board. It uses the facts and results from the other core analytical techniques to determine the most important reasons for the accident.
- Methods: Common methods include the “five whys” (repeatedly asking “why”), analytical trees (such as MORT – Management, Oversight, and Risk Tree, useful for complex accidents), and compliance/noncompliance techniques. “Tier diagramming” is also mentioned.
- Identifying Systemic Root Causes: This involves reviewing causal factors, looking for relationships, grouping related causal factors, and summarizing them into statements that reflect management system deficiencies. These deficiencies often represent failures to properly implement the principles and core functions of Integrated Safety Management (ISM). A Root Cause Worksheet is used to document direct, root, and contributing causes and assign ISM categories.
- Emphasis: Correcting root causes not only prevents the same accident but also addresses wider deficiencies in line management, oversight, and management systems that could cause other accidents. “Inattention to detail” or “not following procedures” are not considered root causes; rather, they are symptoms of deeper systemic issues.
5. Verification Analysis
Verification analysis is a crucial step to ensure the quality, accuracy, and consistency of the investigation results and conclusions.
- Purpose: To verify that the Judgments of Need (JONs) are consistent with the facts, analyses, and causal factors, eliminating irrelevant information and identifying unsupported conclusions.
- Process: Involves working backward through the investigation’s logical flow, ensuring that each JON is tied to at least one causal factor, that causal factors are linked to analyses, and that analyses are linked to facts. Any inconsistencies identified must be resolved, or the unsupported JON removed.
Integration of Human Performance Improvement (HPI) and Integrated Safety Management (ISM)
The EIP methodology integrates HPI and ISM throughout the investigation process.
- Human Performance (HP): The approach recognizes that human error is not the cause of failure, but rather the effect or symptom of deeper trouble in the system. It emphasizes that human error is systematically connected to features of people’s tools, tasks, and the operating environment. Investigations must focus on “why actions of the individuals made sense to them at the time,” rather than simply blaming.
- Error Precursors (TWIN): Unfavorable factors embedded in the job site that increase the chance of error. These are categorized into Task Demands, Work Environment, Individual Capabilities, and Human Nature (TWIN).
- Latent Organizational Weaknesses: These are “unrecognized or undetected deficiencies in an organization’s mission, goals, policies, processes, and programs” that set the stage for errors and determine the severity of consequences. Systemic root causes are often identified as these latent weaknesses.
- Integrated Safety Management (ISM): ISM provides the framework for evaluating management systems and identifying their deficiencies as contributors to accidents.
- Core Functions: The five core functions of ISM (Define the Scope of Work, Identify and Analyze the Hazards, Develop and Implement Hazard Controls, Perform Work within Controls, and Provide Feedback and Continuous Improvement) are used to evaluate how work should be managed safely and to identify deficiencies.
- Guiding Principles: The seven guiding principles of ISM define the characteristics of a safe organization, and deficiencies in their implementation are often contributing or root causes of accidents.
- Organizational Culture: The methodology emphasizes examining leadership, employee engagement, and organizational learning as principal culture-shaping factors to identify cultural issues that contribute to events. A “Just Culture” is promoted, distinguishing between willful violations and unintentional errors to encourage reporting and learning rather than blame.
Reporting and Judgments of Need
The investigation culminates in an accident investigation report that clearly and concisely conveys the results, explaining what happened, why it happened (causal factors), and what can be done to prevent recurrence (JONs). The report must identify both individual and organizational causes and demonstrate that JONs are based on objective analysis and core analytical techniques.
- Judgments of Need (JONs): These are managerial controls and safety measures deemed necessary to prevent or minimize the probability or severity of recurrence. JONs must be linked to causal factors, logically flow from conclusions, and be stated clearly and concisely so they can form the basis for corrective action plans. They should focus on processes and systems, not individuals, and avoid being overly prescriptive or punitive.
By following this comprehensive methodology, the EIP accident investigation aims to provide a deep understanding of accident causation, fostering a continuous learning environment to enhance quality, safety, and productivity in construction and other high-hazard operations.